文献: Velentgas P, Dreyer N, Nourjah P, Smith S, Torhia MM, ed : Developing a protocol for observational comparative effectiveness research: a User’s guide. AHRQ, 2013, Rockville. PubMedリンク
比較効果研究Comparative Effectiveness Research (CER)のNAM National Academy of Medicine (旧IOM Institute of Medicine)の定義は、“比較効果研究CERは臨床状態の予防、診断、治療、モニターのためあるいはケアの供給を改善するための方法の選択肢の益と害を比較するエビデンスの生成と統合を行うことである。CERの目的は個人および集団の両方で、消費者、臨床家、購入者と政策決定者が、ヘルスケアを改善するであろう、情報を与えられた上での決断を支援することである。”です。以前の投稿で述べたとおりです。
一方、診療ガイドラインのMindsの定義は、WHOやGRADE Working groupと同じですが、”診療上の重要度の高い医療行為について、エビデンスのシステマティックレビューとその総体評価、益と害のバランスなどを考量して、患者と医療者の意思決定を支援するために最適と考えられる推奨を提示する文書”です。(Minds診療ガイドライン作成マニュアル2017」)
文献:——– Asche CV ed.: Applying Comparative Effectiveness Data to Medical Decision Making: A Practical Guide. 2016, Adis (Springer International Publishing Switzerland) この本にはCERの定義について、IOMだけでなく、NIH、AHRQ、PCORI、Federal Coordinating Council for Comparative Effectiveness Researchの定義も記載されています。
*もともとIOMは2011年の時点で、システマティックレビューの定義のなかで、システマティックレビューは”scientific investigation”科学的研究であると述べています。 ”A systematic review is a scientific investigation that focuses on a specific question and uses explicit, preplanned scientific methods to identify, select, assess, and summarize the findings of individual, relevant studies. ” (Clinical Practice Guidelines We Can Trust, 2011) また、多くのシステマティックレビュー/メタアナリシスの論文がさまざなジャーナルに発表されていて、システマティックレビュー/メタアナリシスは学問的な活動の成果であることについては異論はないと思います。さらに、CERの条件にあえば、CERとしても成立します。
SOLOとはStructure of Observed Learning Outcomesのことです。知識や技能の浅い理解から深い理解への分類で理論ではなく、エビデンスに基づく分類体系です。学習者が知識や技能を獲得していく過程の研究から生まれたものです。1982年のBiggsとCollisを嚆矢とします( Biggs JB, Collis KF: Evaluating the Quality of Learning: The SOLO taxonomy. 1982, New York: Academic Press. )。カリキュラムを作成する際に用いるタキソノミーすなわち分類体系と呼ばれるもののひとつです。
他には理論に基づくBloom’s taxonomyというのが知られています。(Bloom BS, Engelhart MD, Furst EJ, Hill WH, Krathwohl DR (Eds): Taxonomy of Educational Objectives: The classification of Educational Goals – Handbook 1 Cognitive Domain. 1956, David McKay, New York, NY, USA. )こちらの方は、 知識の形式と知識の獲得・利用とが同列に扱われていることが問題点として指摘されています。
Hook & Millsはその著書で、SOLO taxonomyを用いることで、以下のことが実現できると述べています。 学習者と教師は •学習企図と学習経験を思慮深くデザインできる。 •有効な方略と成功の基準を決めて、用いることができる。 •学習アウトカムのフィードバックと事前のアセスメントを提供することができる。 •次に何をすべきかについて意味のある振り返りができる。 (Hook P, Mills J: SOLO Taxonomy: A guide for Schools BK1: A common language of learning. 2011, Essential Resources Educational Publishers Limited, Laughton, UK. Hook P, Mills J: SOLO Taxonomy: A Guide for Schools. Planning for differentiation. Book 2. 2011, Essential Resources Educational Publishers Limited, New Zealand. )
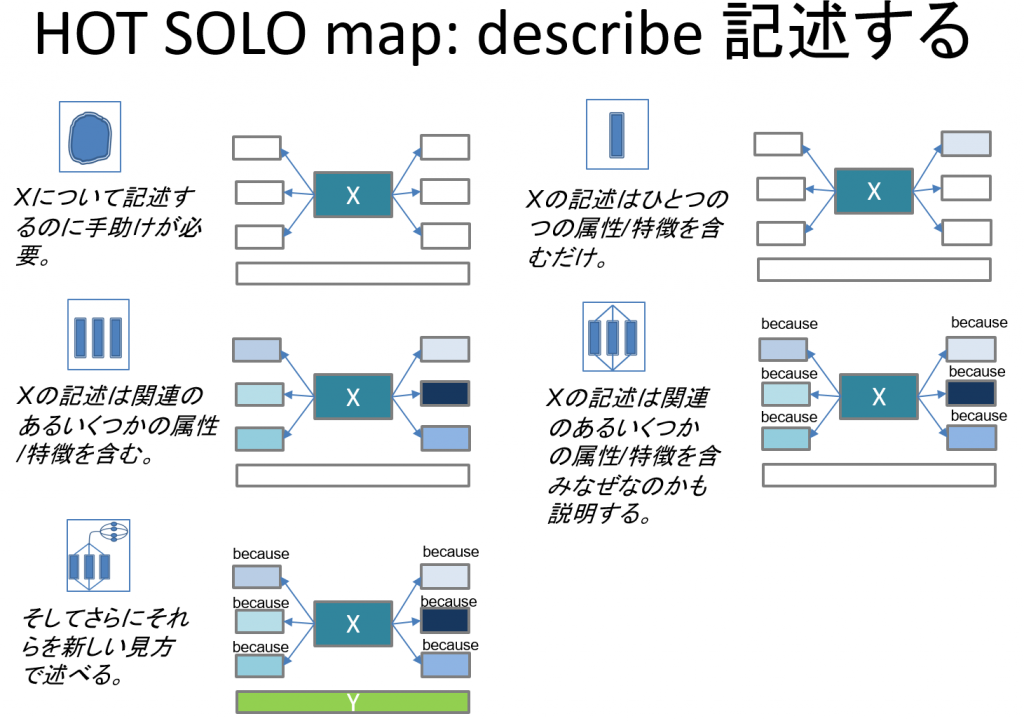
SOLO taxonomyでは学習アウトカムあるいは学習目標を以下の図および表に示すように分類します。アウトカムあるいは目標は知識だけでなく技能、態度にも適用できるはずです。
Guidelines and Economists Network International ( GENI )という国際的組織があります。そのAgenda課題は、
” To facilitate the effective integration of Clinical Practice Guidelines (CPGs), economic and clinical evidence into national decision making and clinical practice in the health sector, especially hospitals and primary care. “
GENIの Chair: Michael Drummond (UK) CEO: Kathryn M. Antioch (Australia) とBoard Members: Louis Niessen (USA) 、 Hindrik Vondeling (Denmark) らの論文が2017年に発表されており、”Economic evidence”を”Clinical Practice Guideline”と”National decision making”にどのように取り入れるかについて、オーストラリアでの体験を踏まえて、述べています。
こちらの論文です。 Antioch KM, Drummond MF, Niessen LW, Vondeling H: International lessons in new methods for grading and integrating cost effectiveness evidence into clinical practice guidelines. Cost Eff Resour Alloc 2017;15:1 DOI 10.1186/s12962-017-0063-x. PMID: 28203120
Economic evidenceはCost-effectiveness analysis (CEA) thresholds, Opportunity cost, Willingness-to-pay (WTP)に関するものです。ただし、End-of-life therapiesは特別の考慮が必要とされます。さらに、”Involvement time, logistics, innovation price, price sensitivity, substitutes and complements, absenteeism and presentismに関わってきます。
Economic evidenceのグレーディングにはThe Consolidated Guidelines for the Reporting of Economic Evaluations (CHEERS) 24 item check listとthe Drummond ten-point check listおよび結果をスコア化するための質問票を用いることを提案しています。(CHEERSとその日本語訳については別の投稿で紹介しました)
この論文のTable 1 Assessing CEA evidence using shadow prices in Australia: NHMRC*ではRanking of evidence on costsとRanking of evidence on effectsの組み合わせで、生存年あたりの費用($)によって推奨する/推奨しないという判定の基準が示されています。(*National Health and Medical Research Council)
そして、”Priority setting remains essential and trade-off decisions between policy criteria can be based on MCDA, both in evidence based clinical medicine and in health planning.” すなわち、「優先度の設定は必須であり、方針基準の間のトレードオフのある意思決定はMCDA(Multi-Criteria Decision Analysis)をよりどころにできるであろう」と述べています。MCDAについてはISPORのGood Practice Guidelines for conduction MCDAの論文、Thokala P 2016とMarsh K 2016が引用されています。(以前の投稿で紹介しました。)
Willingness to pay per QALYまたはLYG (life years gained)の受け入れ可能な最大値(閾値)を設定することで、Cost-Effectiveness Analysis (CEA)のDecision ruleを設定できるのではないかと述べられています。その最大値は、患者と家族のQOL, 生存の改善、機能的状態、重篤でまれで予防可能であるいは若年で永続的な効果につながるか、他の選択肢がない、その介入が平等の見地から他のセクションへの有害な流れを防止できる、などの項目を検討したうえで、妥当性が検討されます。
また、International Health Economists Association (iHWA )という組織があり、2019年7月13-17日スイスBaselで学会が開催されます。そのミッションは以下のとおりです。医療経済学の発展が大きな目的のようです。
“iHEA’s mission is to: Increase communication among health economists; Foster a higher standard of debate in the application of economics to health and health care systems; and Assist young researchers at the start of their careers. “